

Abstract
Background
Treatment advances in the last 10 years, especially the wide use of IMiDs and PI based combinations, have greatly improved the outcomes of patients with multiple myeloma (MM). To understand better the performance of available combination of IMiDs and PIs in the real-world setting, we performed secondary data analyses of two observational studies: FlatIron (Miksad, Clin Pharm Ther, 2018) and Multiple Myeloma Research Foundation (MMRF) CoMMpass study (Miller, Blood Cancer J, 2017). In addition, the MMRF dataset provides patients baseline gene expression and mutation profiles, allowing us to investigate potential correlations between certain biomarkers and drug side-effects.
Methods
We selected NDMM pts who received VRd or KRd as the first line treatment: 1952 pts for VRd and 43 for KRd in Flatiron as of April 30, 2018; while 297 pts for VRd and 63 for KRd in CoMMpass (with patient ID limited to earlier than MMRF_2700 to exclude a subgroup of new patients with limited follow-up). The Flatiron pts were mostly from community hospitals while CoMMpass pts from academic centers, thus these data sets were analyzed separately. Duration of treatment (DOT, a frequently used proxy for PFS in observational studies) was used to evaluate drug treatment effects. DOT was estimated using Kaplan Meier method. Difference between survival curves was tested for statistical significance using the two-sided log-rank test. In addition, differentially expressed genes were identified for MMRF patients by comparing baseline gene expression between responders (VGPR or better) and sub-optimal-responders (PR + SD + PD) patient sub-groups, for KRd and VRd, respectively. Any gene with a t.test p-value < 0.05 and fold-change > 2 between the two groups is considered as a differentially expressed gene. These genes were subsequently evaluated through pathway and Open Targets analysis.
Results
Analysis of the Flatiron dataset showed that baseline characteristics were comparable between patients treated with KRd and VRd (age, gender, race, median BSA, ECOG, hemoglobin, platelets, creatinine clearance, albumin, ISS stages, and beta2-macroglobulin). Similarly, in the MMRF dataset the baseline characteristics were comparable between KRd and VRd pts except for age (median age at 62 for VRd vs 59 for KRd, p-value = 0.00013), creatinine (median at 88.4 µmol/L for VRd vs 78.7 µmol/L for KRd, p-value = 0.03) and hemoglobin (median at 6.76 mmol/L for VRd vs 7.32 mmol/L for KRd, p-value = 0.0018).
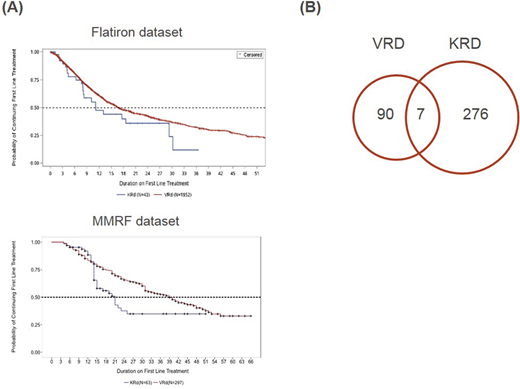
Analysis of the Flatiron dataset showed a median DOT (Figure A) with VRd of 16.81 months (95% CI: 15.69, 19.11) and 11.12 months (95% CI: 8.06, 29.21) with KRd. A comparison of the two treatments show a hazard Ratio (HR, 95% CI, p-value) for VRd vs KRd are: HR = 0.75, CI = (0.49, 1.14), p-value = 0.18. A similar observation was done using the MMRF dataset (Figure A). Here the median DOT for VRd was 39 months (95% CI: 32, 47) while for KRd was 21 months (95% CI: 15, NA) months. The hazard ratio for VRd vs KRd was: HR = 0.61, (95% CI: 0.41, 0.90), p-value = 0.01.
Taken together these observations suggests that in real world the benefits gained by VRd treatment are larger than KRd treatment in NDMM patients.
Although both bortezomib and carfilzomib are proteasome inhibitors, they are chemically different and while bortezomib is a reversible inhibitor, carfilzomib is not. To investigate the molecular characteristics of the responder and sub-optimal-responders treated with these two therapies, we used the baseline gene expression profiles from the MMRF dataset to identify VRd or KRd sensitivity related genes: 97 and 283 genes were identified as differentially expressed genes between drug-responder and sub-optimal-responder groups for VRd and KRd, respectively (Figure B). Pathway and Open Targets analysis were performed on these genes to generate hypotheses for the molecular bases for drug sensitivity as well as observed adverse events such as cardiac side-effects (results will be presented at ASH).
Conclusions
From two observational studies, it appears that VRd leads to longer DOT than KRd in the first line treatment for NDMM patients. Also, drug sensitivity related genes were identified which would help better understand differential efficacy and side-effects. A key limitation of this analysis is the smaller number for KRd pts due to more recent carfilzomib approvals, and longer follow up is needed to confirm these observations.
Li:Takeda Pharmaceuticals International Co.: Employment. Ren:Takeda Pharmaceuticals International Co.: Employment. Shen:Takeda Pharmaceuticals International Co.: Employment. Hou:Takeda Pharmaceuticals International Co.,: Employment. Su:Takeda Pharmaceuticals International Co.,: Employment. Di Bacco:Takeda Pharmaceuticals International Co.: Employment. Hong:Takeda Pharmaceuticals International Co.,: Employment. Galaznik:Takeda Pharmaceuticals International Co.: Employment. Dash:Takeda Pharmaceuticals International Co.: Employment. Crossland:Takeda Pharmaceuticals International Co.: Employment. Dolin:Takeda Pharmaceuticals International Co.: Employment; Shire: Other: PD holds shares in Shire ; GSK: Other: PD holds shares in GSK. Szalma:Takeda Pharmaceuticals International Co.,: Employment; Johnson and Johnson: Other: share holder.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal